

Noo was born with Hirschsprung’s Disease and was diagnosed when he was 16 days old. He had his first surgery, a total collectomy (where they removed 99 % of the colon) when he was 19 days old. He had an ileostomy bag till he was 11 months old when he had his pull through surgery, where they pull the small intestine down to the remaining colon and rectum. The procedure he had is called the Lester Martin pull though (AKA a modified Duhamel procedure). Both surgeries, and all subsequent treatment, were performed by Professor Peter Beale.
28 May 2009 – Specialist Appointment
3 June 2009 – Specialist Appointment update
11 June 2011 – Medical research project developing a new treatment for Hirschsprung’s disease
5 October 2012 – Trip to the ER thanks to Hirschprung’s Disease
10 October 2012 – Noo’s Appointment with the Prof
Bristol Stool Chart
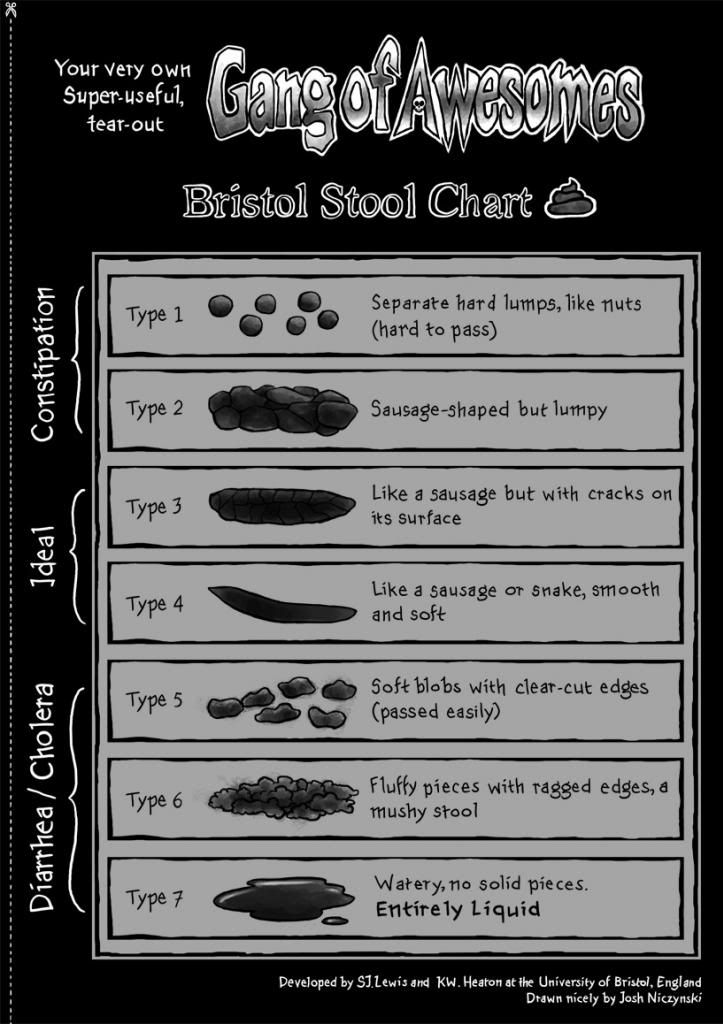
To save this image, right click, select save image as and save
What is Hirschsprung’s Disease
Here is an explanation of on Hirschprung’s disease taken from the John Hopkins Hirschprung’s Disease research website.
What is Hirschsprung disease?
Hirschsprung disease (abbreviated as HSCR) is a developmental problem of the gastrointestinal tract that is present from birth. Hirschsprung disease affects about 1/5000 births, though this rate varies two-fold across the world for reasons still not fully understood.
What causes Hirschsprung disease?
The entire gastrointestinal tract is lined by a complex system of nerve cells (100 million of them)! Some of these nerve cells are responsible for sensing and others are responsible for the motility of the gut. Together they comprise a system capable of detecting material going through and then causing the wave-like contraction and relaxation necessary for passing stool. They also regulate absorption, secretion, and blood flow. These nerve cells are integrated with the rest of the nervous system by way of many neural connections.
HSCR arises early in the embryo when certain nerve cells in the gut (called ganglion cells) fail to develop and mature correctly. Ganglion cells arise from very early specialized cells called neural crest cells, which migrate to the gut and then develop into neurons. In Hirschsprung disease, the cells may fail to migrate, or, normal migration may occur with a subsequent failure of the cells to survive, proliferate, or develop correctly. This results in an ‘aganglionic’ segment (a segment lacking ganglion cells), in which contraction and relaxation is absent, making it difficult for stool to pass through. This leads to chronic constipation and the other symptoms of HSCR.
In HSCR the ganglion cells are missing along varying lengths of the gastrointestinal tract, from the rectum to the small intestine. The anus (the farthest end of the gastrointestinal tract) is almost always affected. About 80% of individuals with Hirschsprung disease have “short-segment” disease, affecting the rectum and sigmoid colon (see diagram below). The other 20% have “long segment” which can include part of the large intestine, the total colon, or even extend to parts of the small intestine. (Note: There are different definitions of long segment Hirschsprung disease. Some define it as lack of ganglion cells in the intestine past the sigmoid region, and others say it means beyond the descending colon/splenic flexure. (See diagram below)
What are the symptoms of Hirschsprung disease?
Hirschsprung disease is most often diagnosed within the first week after birth. However, some individuals are diagnosed later in childhood and as adults, though they have had chronic problems their whole lives. Symptoms of Hirschsprung disease include constipation, abdominal distension, vomiting, decreased appetite, cramping, and failure to thrive. One of the first signs in a newborn is failure to pass meconium (the first bowel movement) within 24-48 hours after birth. Some infants also develop enterocolitis, an acute inflammation of the bowel requiring immediate medical attention. Signs of enterocolitis are diarrhea and fever.
How is it diagnosed?
There are several diagnostic tools used to diagnose Hirschsprung disease:
- Barium enema x-ray: Barium, a chalky liquid, is inserted through the anus into the colon, and coats the inside of the colon. When an x-ray of the abdomen is taken, this part lights up. If Hirschsprung disease is present, a “transition zone” may be apparent. In the segment without nerve cells, the colon will appear to be of normal size or somewhat constricted. In the area above, however, the colon will appear dilated. The stool that cannot be passed backs up and the colon is stretched and enlarged. Visualizing the funnel-like transition zone is a clue that that individual may have Hirschsprung disease.
- Rectal biopsy: The definitive diagnosis of Hirschsprung disease is made by a rectal biopsy. This procedure involves removing a small piece of tissue from the rectum. Doctors examine the tissue sample under a microscope and look for the presence of ganglion cells (nerve cells). If no nerve cells are visualized, Hirschsprung disease is diagnosed. During surgery, serial intestinal biopsies are performed by a pathologist, so that the transition zone can be precisely located.
- Rectal manometry: The doctor inflates a small balloon inside the rectum. Normally, the anal muscle will relax. If it doesn’t, HD may be the problem.
How is it treated?
Treatment for Hirschsprung disease consists of surgery to remove the affected segment and re-connect the remaining intestine to the anus so stool can pass out of the body. This is called a “pull-through” surgery. There are various surgical techniques and methods in clinical use. Some patients may need a temporary or permanent ostomy (opening to the outside of the body by a hole in the abdomen, through which stool passes), as part of surgical treatment.
The long-term outcome of surgery for Hirschsprung disease is generally good, with the majority of patients having normal or almost normal bowel habits. Some individuals do experience continuing problems with frequency of bowel movements, constipation/diarrhea, bowel incontinence, and recurrent episodes of enterocolitis.
Famous people with Hirshprung’s Disease
Elvis Presley
